Apex Beat Guide: Tapping vs. Heaving, Displacement & Clinical Causes
In this era of high-tech Echocardiography and MRI, it is easy to undervalue the humble physical examination. But the Apex Beat offers us something no machine can: a direct physical handshake with the heart.
The Apex Beat (or Point of Maximal Impulse – PMI) is the only point where the heart directly touches the chest wall. By simply placing your hand on the precordium, you are palpating the very mechanics of the cardiac cycle. It is not just an anatomical location… it is a gateway to diagnosing pressure overloads, volume overloads, and valvular pathologies.
What is the Apex Beat?
Clinically, the apex beat is defined as the lowermost and outermost (most inferior and lateral) prominent cardiac pulsation in the precordium.
The Mechanism: Why does it tap?
One of my students recently asked a pertinent question:
“Sir, when the heart contracts, it expels blood up towards the aorta (the base). So why does the apex beat move ‘outward’ against the chest?”
The answer is in the anatomy of the heart. The cardiac muscle is arranged in a spiral syncytium. When it contracts, the heart produces a torque, i.e., it rotates counter-clockwise. This rotation swings the apex forward, causing it to give a feeling of “tap” against the chest wall.
How to Locate the Apex Beat
Accuracy is everything here. Do not guess.
- The Standard: In a healthy adult, the apex beat is located in the left 5th intercostal space, about 1 cm medial to the mid-clavicular line (MCL).
- The Reference: Always use the MCL (the midpoint between the sternoclavicular and acromioclavicular joints). Do not measure from the sternum or the nipple, as these landmarks vary too much between patients.
The Pediatric Rule
Be careful with children. In children under 7 years of age, the heart is placed higher. You will find the apex beat in the 4th intercostal space, just lateral to the MCL.
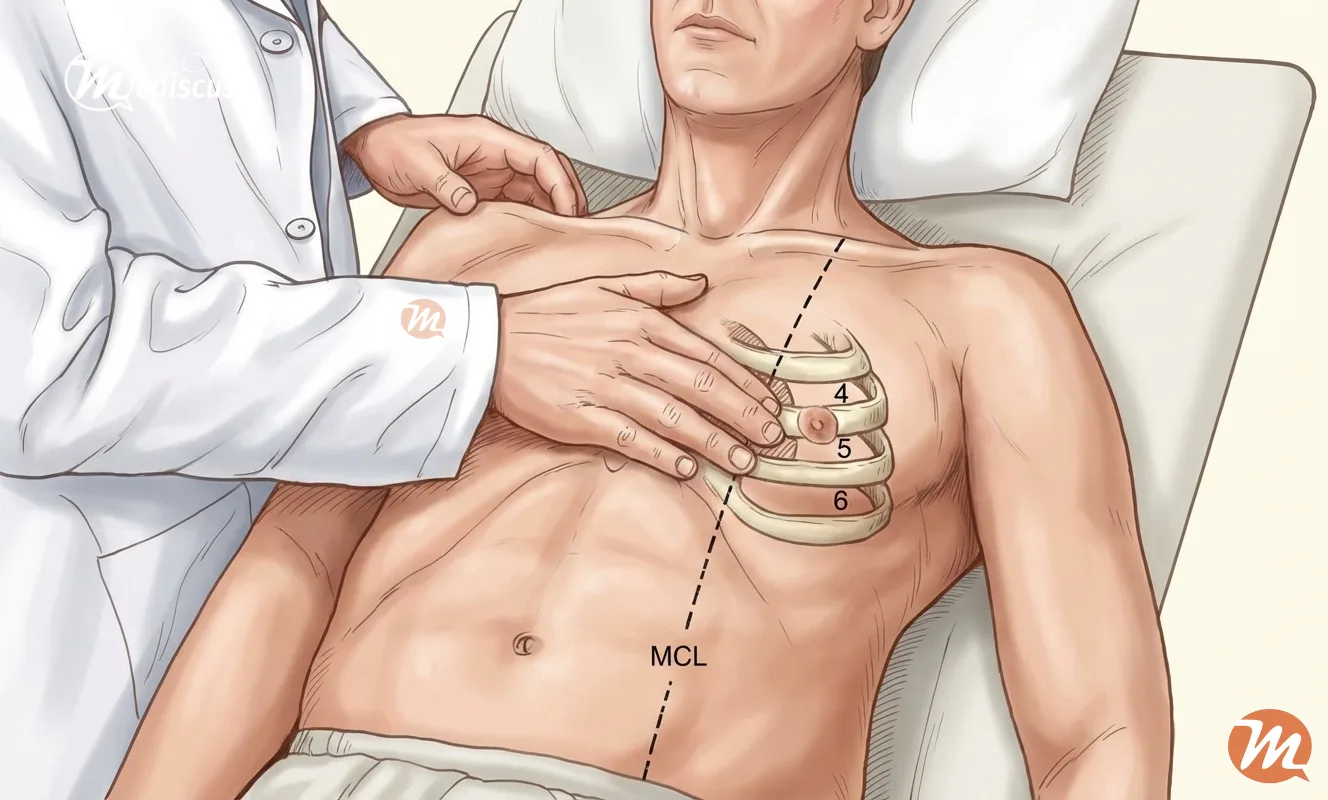
The Examination Method
- Start wide: Place the flat of your hand over the left side of the patient’s chest (covering the 4th, 5th, and 6th intercostal spaces).
- Pinpoint: Once you feel the general pulsation, switch to your middle finger to localize the exact point of maximal impulse.
- Verify: Palpate the sternal angle (angle of Louis). This corresponds to the 2nd rib. Slide down to the space below it (2nd intercostal Space) and count down to the 5th space to confirm your location.
Clinical Pearl: Why can’t I feel it?
You have palpated carefully, but you feel nothing.
Before you panic, run through the DR POPE mnemonic.
DR POPE: Causes of an Absent Apex Beat
- D – Dextrocardia (Check the right side!)
- R – Rib (The apex might be hiding directly behind a rib; turn the patient to the left lateral position).
- P – Pericardial Effusion (Fluid masks the beat).
- O – Obesity (Thick chest wall dampens the impulse).
- P – Pleural Effusion (Left-sided fluid pushes the heart away).
- E – Emphysema (Hyper-inflated lungs cover the heart).
Interpreting Displacement
If the apex beat is palpable but not where it should be, the direction of displacement tells you the pathology.
First, check the Trachea. If the trachea is deviated, the heart is being pushed or pulled by lung pathology (e.g., fibrosis, collapse, or pneumothorax).
If the trachea is central, the displacement is likely cardiac:
- Downwards & Lateral: Suggests Left Ventricular Enlargement (The LV grows down).
- Lateral Only: Suggests Right Ventricular Enlargement (The RV pushes the LV sideways).
The Diagnostic Table: Character of the Beat
This is the most critical skill to master. Don’t just find the beat… describe it. Is it tapping? Heaving?
 Apex Beat Diagnostic Guide
Apex Beat Diagnostic Guide| Type of Beat | What it Feels Like | The Underlying Cause |
|---|---|---|
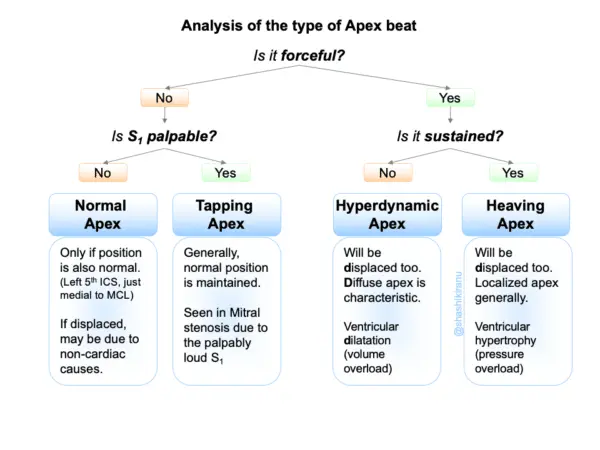
| Normal | A gentle, localized lift (area < 2-3cm). | Healthy Heart. |
| Tapping | A “short, sharp shock.” Feels like a fingertip tapping you. | Mitral Stenosis. (The tap is actually the palpable, loud First Heart Sound – S1). |
| Heaving | A forceful, sustained thrust that lifts your finger for a noticeable duration. | Pressure Overload (e.g., Aortic Stenosis, Systemic Hypertension, LV Hypertrophy). |
| Hyperdynamic | Forceful but ill-sustained (short duration). Often diffuse (>3cm). | Volume Overload (e.g., Aortic Regurgitation, Mitral Regurgitation, High Output States). |
| Double Impulse | Two distinct hits per beat. | HOCM (Hypertrophic Cardiomyopathy). The stiff ventricle causes a palpable S4. |
| Dyskinetic | Uncoordinated, “wobbly” motion. | Ventricular Aneurysm (post-MI). |
Palpable in a single intercostal space. The diameter is < 3 cm (usually 2-3 cm).
Palpable in more than one space OR the diameter is > 3 cm (even if in one space).
An Algorithm: Analyzing the Apex Beat
Key Takeaways
- The Definition: Lowermost, outermost point of definitive pulsation.
- The Location: 5th ICS, medial to MCL (Adults). 4th ICS (Children <7).
- The Distinction: Heaving = Pressure (Hypertension). Hyperdynamic = Volume (Regurgitation).
- The Trick: If you can’t feel it, turn the patient to the left (to rule out rib placement), then think of DR POPE.
Mastering the apex beat takes practice. Next time you are on rounds, don’t just put your stethoscope on the chest… palpate with your hand first.
Dr. Shashikiran Umakanth (MBBS, MD, FRCP Edin.) is the Professor & Head of Internal Medicine at Dr. TMA Pai Hospital, Udupi, under the Manipal Academy of Higher Education (MAHE). While he has contributed to nearly 100 scientific publications in the academic world, he writes on MEDiscuss out of a passion to simplify complex medical science for public awareness.









